Presentation of Case
A 37-year-old woman was admitted to the general ward yesterday because of syncope.
This patient had been in her usual state of health until one day before this admission, when syncope occurred while swimming. The lifeguard, who witnessed the event, reported that 「she developed loss of consciousness and sank to the bottom of pool.」 She was rescued right away, and, after a few seconds, she had regained consciousness and recovered fully. She claimed that she experienced neither palpitations nor any prodromal symptom. She denied of taking any medications, but she reported that her brother had sudden cardiac death at the age of 25 years. Her cousin brought her to ER for further evaluation and treatment immediately.
On physical examination, the patient』s vital signs were normal, with the heart rate of 75 beats per minute that was regular, the blood pressure of 123/80 mmHg, and the temperature of 36.5°C. The thyroid was normal in size, with no palpable nodules. No heart murmur was noted. The remainder of the physical examination, including neurologic exam, was normal.
Chest X-ray showed no cardiomegaly and no definite lung lesions. Her resting EKG was interpreted as normal sinus rhythm with prolonged QT (QTc = 504 msec) and broad inverted T wave in the leads V2-6. Routine laboratory tests, urinalysis, and thyroid function tests were performed.
< EKG > (Time: December 18th, 2012)
< Pedigree >
<Laboratory data>
CBC/DC: (Time: December 18th, 2012)
WBC, /μL |
6800 |
Blast, % |
0 |
Mono, % |
2 |
RBC, M/μL |
4.5 |
Promyel, % |
0 |
Lym, % |
0 |
Hb, g/dL |
13.5 |
Myelo, % |
0 |
Aty. lym, % |
0 |
Hct, % |
40.5 |
Meta, % |
0 |
Plasma cell, % |
0 |
MCV, fl |
90.3 |
Band, % |
0 |
|
|
PLT, /μL |
370000 |
Seg, % |
10 |
|
|
|
|
Eos, % |
0 |
|
|
|
|
Baso, % |
0 |
|
|
Biochemistry: (Time: December 18th, 2012)
BUN, |
mg/dL |
10.0 |
Na, |
mmol/L |
136 |
Cre, |
mg/dL |
0.7 |
K, |
mmol/L |
4.1 |
T-Bil, |
mg/dL |
0.62 |
Ca, |
mmol/L |
2.29 |
ALT, |
U/L |
21 |
Mg, |
mmol/L |
0.85 |
Urinalysis: (Time: December 18th, 2012)
SpGr |
|
1.013 |
RBC, |
/HPF |
0-2 |
pH |
|
5.6 |
WBC, |
/HPF |
0-2 |
Protein |
|
- |
Epi, |
/HPF |
0-2 |
Glucose |
|
- |
Cast |
|
- |
Ketones |
|
- |
Nitrite |
|
- |
OB |
|
- |
Crystal |
|
- |
Hormonal data: (Time: December 18th, 2012)
hsTSH, |
μIU/ml |
1.55 |
fT4, |
ng/dL |
0.82 |
Course and Treatment
Echocardiogram was interpreted as normal left ventricular ejection fraction (M-mode: 63%) without any structural abnormalities. Genetic testing showed that the patient had a missense mutation (G643S) in KCNQ1 gene (LQT1 gene). Bisoprolol (5 mg, 1/2# qd) was given and an implantable cardioverter-defibrillator (ICD) was implanted. EKGs and genetic testing were obtained on all live first-degree family members, which were reported to be normal.
Discussion
這位病人主要的主訴為syncope,針對一位年輕女性syncope的鑑別診斷可分為四大類:
- Vasovagal: 咳嗽、大小便等
- Orthostatic hypotension: hypovolemia、diuretics、vasodilators等
- Cardiovascular: arrhythmia如sick sinus syndrome、high-grade AV block等,mechanical如hypertrophic cardiomyopathy、aortic stenosis、mitral stenosis、tamponade等
- Neurologic: seizure、transient ischemic attack/cerebrovascular accident、vertebrobasilar insufficiency等
在history taking時,這位患者聲稱在syncope之前沒有任何的prodrome,如nausea、diaphoresis、或blurry vision等,也沒有任何的precipitating factors,如姿勢上的改變、壓力源(疼痛、情緒、咳嗽、大小便等),更沒有associated symptoms (胸痛、心悸、大小便失禁、神經學症狀、post-ictal等)。她也提到沒有任何系統性疾病和用藥史,唯一只有她的弟弟在25歲時因sudden cardiac death過世,所以初步推測syncope比較有可能是心因方面的因素造成的。Physical examination沒看到goiter或是聽到heart murmurs,neurologic exam沒有發現neurologic deficits,抽血報告沒有甲狀腺機能異常或電解質不平衡,這些negative findings指出這不太像是metabolism或是神經性的因素造成的syncope。EKG顯示QT prolongation (QTc = 504 msec),讓人在第一時間聯想到long QT syndrome (LQTS)。心臟超音波的結果也是正常的,無結構性的心臟病如hypertrophic cardiomyopathy或AS等。
根據Schwartz et al在1993年發表的long QT syndrome (LQTS)診斷標準
(see Table 1),病患發生syncope (without stress)、EKG上看到的QTc > 500 msec,且她的弟弟在30歲前發生sudden cardiac death,總分有4.5分,所以可以診斷LQTS。
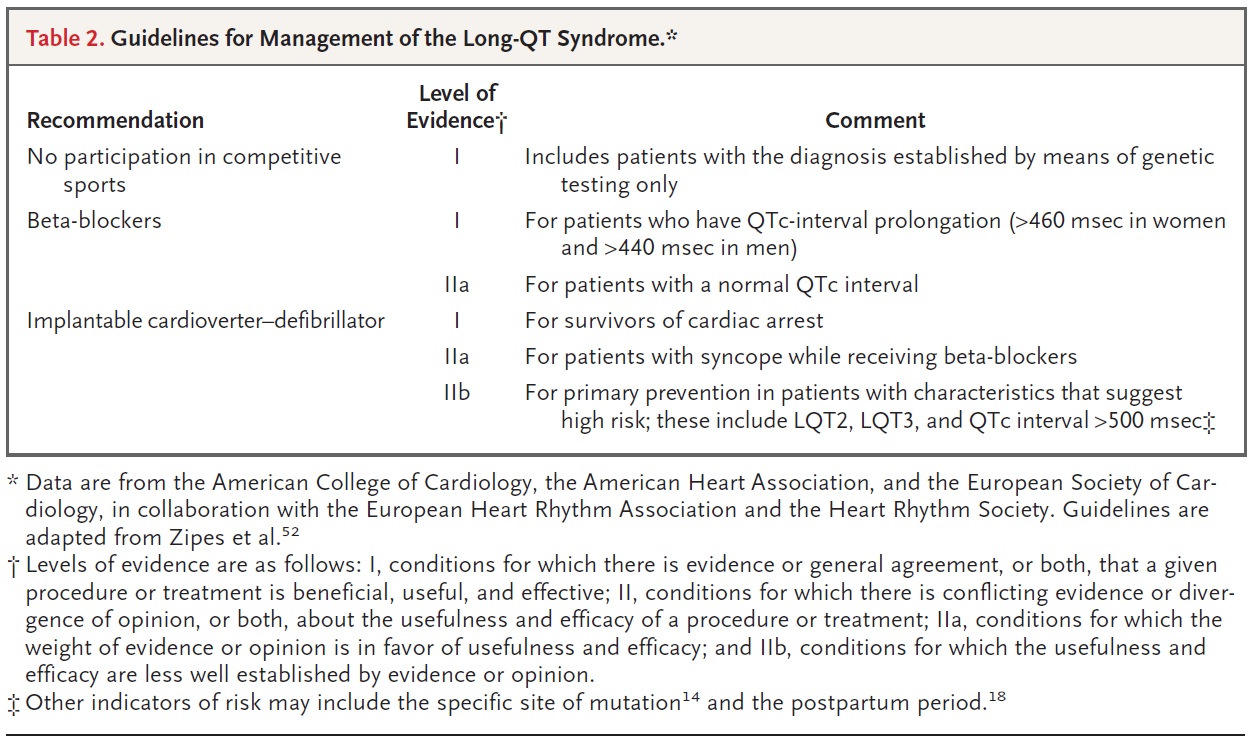
由於病患syncope的發生是在游泳時,聽起來像是典型的LQT1 gene有變異 (See Table 2),經由genetic testing也證實在KCNQ1有missense mutation(第643的氨基酸從glycine變成serine)。除了病患本身的治療外,一等親的家人也強力建議做genetic screening。
Long QT syndrome的介紹
Long QT syndrome (LQTS)是一種先天性的疾病,特徵是在EKG上會看到QT interval prolongation,且很可能導致torsades de pointes、ventricular tachyarrhythmia,進而產生syncope,cardiac arrest,甚至sudden death。
LQTS的好發年齡較偏年輕,但也有可能到中年才有症狀,且女性的發生率比男性高,整體prevalence rate為1:2000-5000。病患常因adrenergic stimuli如運動、情緒、吵雜聲』、游泳等誘發心律不整,但也有是在毫無刺激的情況下就產生心律不整。藥物如erythromycin等也有可能造成LQTS,而這多好發在患者為女性、電解質不平衡(如hypokalemia、hypomagnesemia, hypocalcemia)、低體溫、不正常的甲狀腺功能、結構性的心臟病、心跳過慢等等。
LQTS的原因是心肌的離子通道(如K+、Na+、Ca2+ channels)有genetic mutations,造成離子傳導不平衡,目前在十個基因上發現上百種mutations與LQTS有相關,最常見的基因亞型為LQT1 gene (KCNQ1)、LQT2 gene (KCNH2)、LQT3 gene (SCN5A) (See Table 2)。
LQTS的診斷通常依賴病人的臨床表現及EKG。LQTS常見的臨床表現如前面提到的syncope、cardiac arrest或sudden death。若是本身就被診斷LQTS,或是懷疑家族裡有此遺傳,就算沒有症狀的人也需要被評估。在正常的 resting EKG方面,女性的QTc上限為460 msec,男性則為440 msec。而詳細的家族史也佔了LQTS診斷的重要一環,除了sudden death以外,是否溺水、sudden infant death syndrome、或是開車時死亡也是要釐清的。若懷疑LQTS,首先要先排除藥物(antiarrhythmic agents如sotalol、dofetilide;noncardiovascular drugs如haloperidol、methadone、pentamidine)、電解質不平衡、甲狀腺功能及結構性的心臟病所造成的acquired LQTS。若是病患的臨床表現有syncope或sudden cardiac death,再加上EKG呈現long QT,通常意味著LQTS,進一步可做基因檢測來證實。但是,有時病患的表現並不那麼typical,我們可參考Schwartz et al在1993年發表的LQTS診斷標準(see table 1)。此表將診斷標準分成三個類別,滿分為九分,大於或等於四分則代表LQTS的機率很高。
臨床確診LQTS後,genetic testing在病患和其家屬是建議的(Class I recommendation) (See table 3)。目前可在70~75%的患者中找到mutations,剩下的則可能是因為尚未找到的基因有著罕見的mutation而無法驗出,所以陰性報告不代表此患者沒有LQTS。此外,genetic testing還可釐清預後和治療方式。
LQTS的建議與治療包括了避免劇烈運動、beta-blockers、implantable cardioverter-defibrillator (ICD) (see Table 4)。若是病患是sudden death的高危險群,如青春期前就出現症狀、QTc >500 msec、或是反覆發作的syncope,裝置ICD是建議的。
總而言之,根據此病人的臨床表現(syncope while swimming)、family history(她的弟弟在30歲前發生sudden cardiac death)、EKG(QTc > 500 msec)、實驗室檢查(genetic test: missense mutation (G643S) in KCNQ1 gene (LQT1 gene)),得知此病人的診斷為long QT syndrome且為高風險群,所以除了藥物治療、裝置ICD外,也對其family members做genetic testing,開始追蹤其治療效果。
References:
- Sovari, AA, Rottman JN. Long QT Syndrome Treatment & Managaement. Medscape: http://emedicine.medscape.com/article/157826-treatment#showall
- Roden, DM. Long-QT Syndrome. N Engl J Med 2008;358:169-76.
- Goldenerg, I, Moss AJ. Long QT Syndrome. JACC 2008:51:24:2291-2300.
- Ackerman, MJ, et al. HRS/EHRA Expert Consensus Statement on the State of Genetic Testing for the Channelopathies and Cardiomyopathies. Europace 2011:13:1077-1109.
|
{kind=link}